, or banding, is a commonly used, minimally invasive procedure for treating internal hemorrhoids. For some patients, it can provide symptom relief without surgery. However, like any medical procedure, rubber band ligation has limitations—and understanding its disadvantages is important before deciding if it’s the right treatment option.
If you’re considering rubber band ligation or have already undergone the procedure and are still experiencing symptoms, knowing the potential downsides—and exploring advanced, non-surgical alternatives like Hemorrhoid Artery Embolization (HAE)—can help you make a more informed decision about your care.
Rubber Band Ligation Treats the Hemorrhoid, Not the Cause
One of the main disadvantages of rubber band ligation is that it treats the hemorrhoid itself, not the underlying cause.
Hemorrhoids often develop due to increased pressure and abnormal blood flow in the rectal veins. Rubber band ligation cuts off blood supply to a single hemorrhoid, causing it to shrink and fall off—but it does not address the blood vessels that caused the hemorrhoid to form in the first place.
Because of this, new hemorrhoids can develop over time, even after successful banding.
Explore Long-Term Alternatives to Banding
Hemorrhoid Symptoms Often Return
Another major limitation of rubber band ligation is the risk of recurrence. In fact, a major clinical trial published in The Lancet found that hemorrhoid symptoms returned in 49% of patients within just 12 months of undergoing banding.[1] Because this method doesn’t address the underlying blood supply, symptoms frequently return.
While some patients experience relief after treatment, others may notice:
-
Bleeding returning weeks or months later
-
New hemorrhoids forming
-
Persistent discomfort despite multiple banding sessions
In many cases, patients require repeat treatments, especially if they have more than one internal hemorrhoid or ongoing risk factors such as chronic constipation or prolonged sitting.
Find out if HAE Can Stop Your Recurring Bleeding
Post-Procedure Discomfort Is Common
Rubber band ligation is performed right in a doctor’s office or clinic setting, and the application itself usually takes only a few minutes. Because internal hemorrhoids are located in an area of the rectum that lacks sharp pain-sensing nerves, the procedure is typically done without any local anesthetic, numbing injections, or sedation.
However, “minimally invasive” does not mean entirely pain-free. While patients don’t feel a sharp cutting sensation when the band is applied, they immediately experience a deep, intense feeling of rectal pressure, fullness, or a heavy cramping sensation—similar to the urgent need to have a bowel movement.
Because this is a deep muscular ache rather than surface pain, topical numbing gels do not provide relief. After leaving the office, patients may notice:
-
-
Persistent Rectal Pressure: A dull, heavy ache or cramping that can last for 24 to 48 hours.
-
Difficulty Sitting Comfortably: General pelvic discomfort that makes sitting for long periods difficult for several days.
-
Bleeding Risks: Mild bleeding when the banded tissue finally withers and falls off (usually 5 to 10 days later).
-
Post-procedure discomfort is usually treated by over-the-counter relievers like acetaminophen (Tylenol) and warm sitz baths. Blood-thinning pain relievers like ibuprofen or aspirin must be avoided, as they can increase the risk of bleeding. Discomfort varies from person to person, but for many, the recovery after an office visit can be more uncomfortable and disruptive than expected.
Banding Is Not Suitable for All Types of Hemorrhoids
Rubber band ligation is only effective for internal hemorrhoids.
It is not recommended for:
-
External hemorrhoids
-
Mixed internal and external hemorrhoids
-
Advanced or prolapsed hemorrhoids that cannot be repositioned
Patients with more complex or severe hemorrhoids may not be good candidates for banding and may require alternative treatment options.
Rubber Banding Ligation Risks
While serious complications are uncommon, rubber band ligation does carry some risks, including:
-
Significant pain if the band is placed too low
-
Infection
-
Excessive bleeding
-
Thrombosed hemorrhoids
In rare cases, complications may require additional medical treatment or intervention.
Banding Requires Multiple, Staged Appointments
Rubber band ligation is typically performed on just one hemorrhoid at a time to minimize pain and complications. If you have multiple internal hemorrhoids, this means scheduling several separate appointments spaced weeks apart. For individuals seeking a single-procedure solution that treats the entire area at once—like Hemorrhoid Artery Embolization—the prolonged timeline of banding can be a major drawback.
When Rubber Band Ligation May Not Be Enough
If hemorrhoid symptoms are chronic, severe, or continue after banding, rubber band ligation may not provide long-term relief. Patients who experience ongoing bleeding or recurring symptoms may benefit from a treatment that addresses hemorrhoids more comprehensively.
A thorough evaluation by a specialist is essential to determine whether rubber band ligation is appropriate—or if another minimally invasive option may be better suited.
Hemorrhoid Artery Embolization vs. Rubber Band Ligation

For patients who continue to experience hemorrhoid symptoms or want a more comprehensive treatment approach, it’s helpful to understand how hemorrhoid artery embolization (HAE) compares to rubber band ligation (RBL).
While both are minimally invasive and performed without traditional surgery, they treat hemorrhoids in very different ways.
How the Treatments Differ
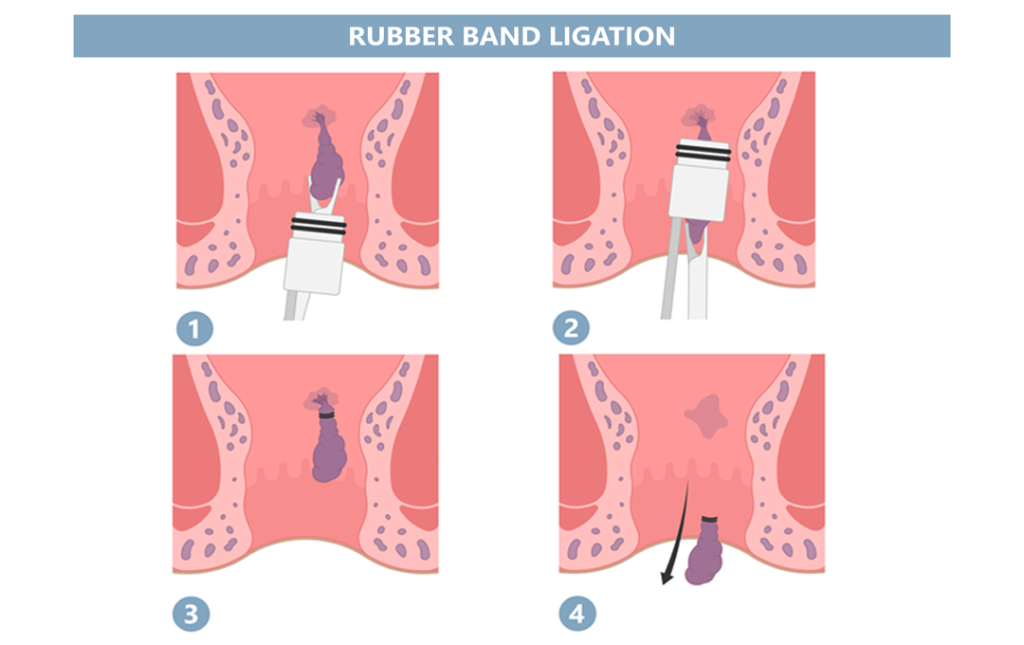
Rubber band ligation works by placing a small rubber band around an individual internal hemorrhoid. This cuts off its blood supply, causing the hemorrhoid to shrink and fall off. The treatment focuses on addressing one hemorrhoid at a time and does not target the underlying blood vessels that contribute to hemorrhoid formation.
Hemorrhoid artery embolization treats hemorrhoids from the inside out. During this outpatient procedure, an interventional specialist inserts a tiny, flexible tube called a catheter through a microscopic pinprick—typically in the wrist or the groin. Using advanced live X-ray imaging, the doctor navigates through the blood vessels directly to the overactive arteries feeding the hemorrhoid. They then place microscopic particles to safely block that excess blood flow. Over time, the hemorrhoids shrink naturally without anything being cut, burned, or banded near the highly sensitive rectal area.
Key Differences to Consider
-
Treatment focus:
Rubber band ligation treats individual hemorrhoids, while hemorrhoid artery embolization addresses the underlying blood supply contributing to hemorrhoid symptoms. -
Pain and recovery:
Rubber band ligation can cause post-procedure discomfort, pressure, or bleeding when the banded tissue falls off. Hemorrhoid artery embolization requires no rectal intervention. Because access is achieved through a tiny pinprick in the arm or leg, it is associated with minimal discomfort and a significantly smoother recovery -
Number of treatments:
Rubber band ligation may require multiple sessions if more than one hemorrhoid is present. Hemorrhoid artery embolization is typically completed in a single procedure. -
Recurrence risk:
Because ligation leaves the main high-pressure pipeline intact, symptoms often return.
Hemorrhoid Artery Embolization Information
Which Option May Be Right for You?
Rubber band ligation may be appropriate for patients with mild to moderate internal hemorrhoids and limited symptoms. Hemorrhoid artery embolization may be a better option for patients with chronic bleeding, recurring hemorrhoids, or those who have not found lasting relief with banding.
A proper evaluation is essential to determine the most appropriate treatment based on symptom severity, hemorrhoid type, and overall health.
Talk to a Hemorrhoid Specialist About Your Options
While rubber band ligation can be effective for some patients, it is not a one-size-fits-all solution. Understanding its disadvantages helps set realistic expectations and ensures you receive the right treatment for your specific condition.
At USA Hemorrhoid Centers, patients receive personalized evaluations to determine the most appropriate approach based on symptoms, hemorrhoid type, and overall health.
Take the Next Step
If hemorrhoids are affecting your quality of life—or if prior treatments haven’t worked—it may be time to explore your options with a specialist. The right treatment plan starts with understanding what works best for you.
Schedule a Consultation Online
1] Brown, S., et al. (2016). “Haemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second-degree and third-degree haemorrhoids (HubBLe): a multicentre, open-label, randomised controlled trial.” The Lancet, 388(10042), 356-364.